

Epidemiology and Outcomes of Hospitalizations With Invasive Aspergillosis in the United States, 2009-2013
- PMID: 29718296
- PMCID: PMC7190884
- DOI: 10.1093/cid/ciy181
Epidemiology and Outcomes of Hospitalizations With Invasive Aspergillosis in the United States, 2009-2013
Abstract
Background: Though invasive aspergillosis (IA) complicates care of up to 13% of patients with immunocompromise, little is known about its morbidity and mortality burden in the United States.
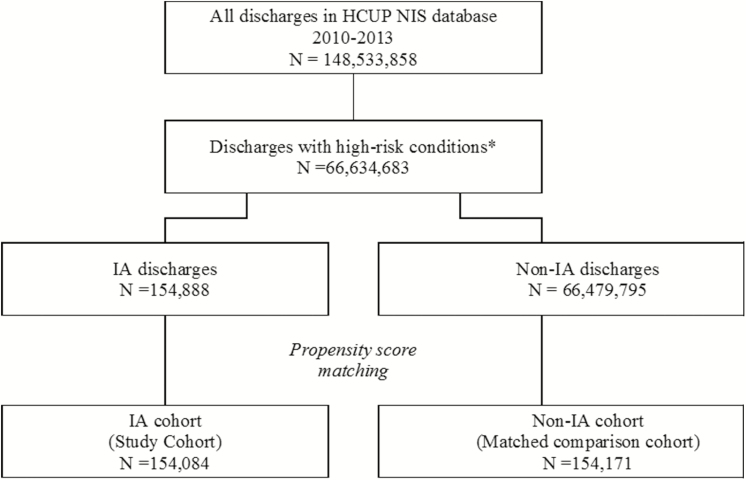
Methods: We analyzed the Health Care Utilization Project's data from the Agency for Healthcare Research and Quality for 2009-2013. Among subjects with high-risk conditions for IA, IA was identified via International Classification of Diseases, Ninth Revision, Clinical Modification codes 117.3, 117.9, and 484.6. We compared characteristics and outcomes between those with (IA) and without IA (non-IA). Using propensity score matching, we calculated the IA-associated excess mortality and 30-day readmission rates, length of stay, and costs.
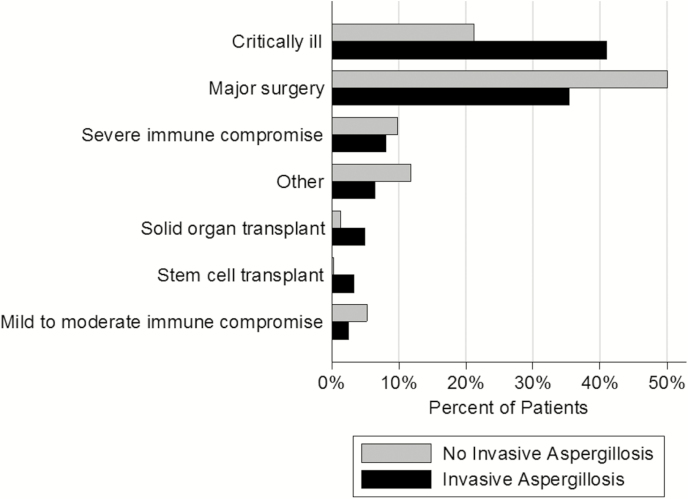
Results: Of the 66634683 discharged patients meeting study inclusion criteria, 154888 (0.2%) had a diagnosis of IA. The most common high-risk conditions were major surgery (50.1%) in the non-IA and critical illness (41.0%) in the IA group. After propensity score matching, both mortality (odds ratio, 1.43; 95% confidence interval, 1.36-1.51) and 30-day readmission (1.39; 1.34-1.45) rates were higher in the IA group. IA was associated with 6.0 (95% confidence interval, 5.7-6.4) excess days in the hospital and $15542 ($13869-$17215) in excess costs per hospitalization.
Conclusions: Although rare even among high-risk groups, IA is associated with increased hospital mortality and 30-day readmission rates, excess duration of hospitalization, and costs. Given nearly 40000 annual admissions for IA in the United States, the aggregate IA-attributable excess costs may reach $600 million annually.
Figures
Comment in
-
Reply to van de Peppel and de Boer.Clin Infect Dis. 2019 Jan 18;68(3):532. doi: 10.1093/cid/ciy699. Clin Infect Dis. 2019. PMID: 30165475 No abstract available.
-
The Complex Case of Aspergillus and Mortality.Clin Infect Dis. 2019 Jan 18;68(3):531-532. doi: 10.1093/cid/ciy698. Clin Infect Dis. 2019. PMID: 30165683 No abstract available.
References
-
- Minari A, Husni R, Avery RK, et al. . The incidence of invasive aspergillosis among solid organ transplant recipients and implications for prophylaxis in lung transplants. Transpl Infect Dis 2002; 4:195–200. - PubMed
-
- Montoya JG, Chaparro SV, Celis D, et al. . Invasive aspergillosis in the setting of cardiac transplantation. Clin Infect Dis 2003; 37(suppl 3):S281–92. - PubMed
-
- Paterson DL, Singh N. Invasive aspergillosis in transplant recipients. Medicine (Baltimore) 1999; 78:123–38. - PubMed
-
- Singh N, Arnow PM, Bonham A, et al. . Invasive aspergillosis in liver transplant recipients in the 1990s. Transplantation 1997; 64:716–20. - PubMed
-
- Marr KA, Carter RA, Boeckh M, Martin P, Corey L. Invasive aspergillosis in allogeneic stem cell transplant recipients: changes in epidemiology and risk factors. Blood 2002; 100:4358–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
