

The Dana-Farber CISNET Model for Breast Cancer Screening Strategies: An Update
- PMID: 29554465
- PMCID: PMC5929104
- DOI: 10.1177/0272989X17741634
The Dana-Farber CISNET Model for Breast Cancer Screening Strategies: An Update
Abstract
Background: We present updated features to a model developed by Dana-Farber investigators within the Cancer Intervention and Surveillance Modeling Network (CISNET). The initial model was developed to evaluate the impact of mammography screening strategies.
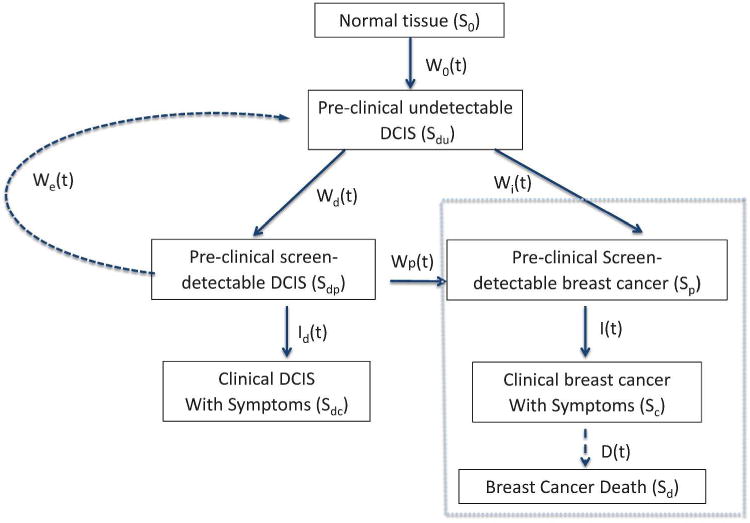
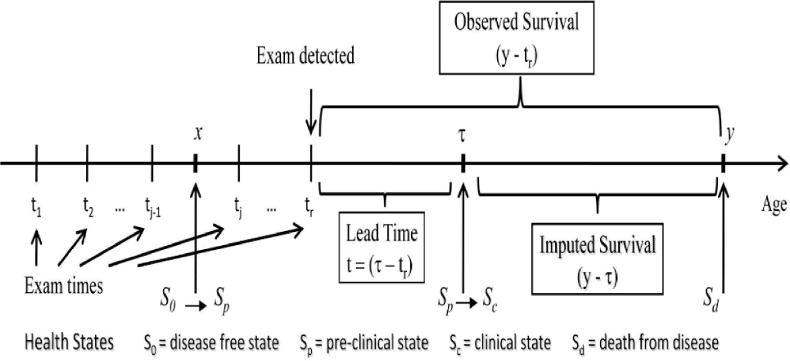
Methods: This major update includes the incorporation of ductal carcinoma in situ (DCIS) as part of the natural history of breast cancer. The updated model allows DCIS in the pre-clinical state to regress to undetectable early-stage DCIS, or to transition to invasive breast cancer, or to clinical DCIS. We summarize model assumptions for DCIS natural history and model parameters. Another new development is the derivation of analytical expressions for overdiagnosis. Overdiagnosis refers to mammographic identification of breast cancer that would never have resulted in disease symptoms in the patient's remaining lifetime (i.e., lead time longer than residual survival time). This is an inevitable consequence of early detection. Our model uniquely assesses overdiagnosis using an analytical formulation. We derive the lead time distribution resulting from the early detection of invasive breast cancer and DCIS, and formulate the analytical expression for overdiagnosis.
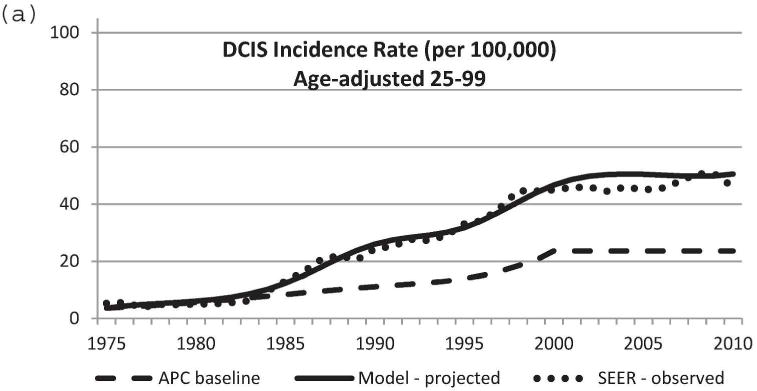
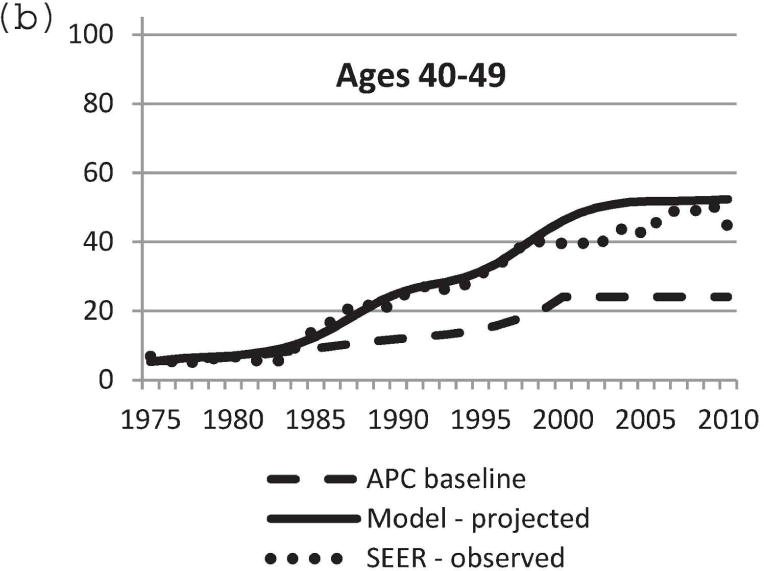
Results: This formulation was applied to assess overdiagnosis from mammography screening. Other model updates involve implementing common model input parameters with updated treatment dissemination and effectiveness, and improved mammography performance. Lastly, the model was expanded to incorporate subgroups by breast density and molecular subtypes.
Conclusions: The incorporation of DCIS and subgroups and the derivation of an overdiagnosis estimation procedure improve the model for evaluating mammography screening programs.
Keywords: ductal carcinoma in situ; lead time; mammography screening; overdiagnosis.
Figures
References
-
- Lee SJ, Zelen M. Scheduling periodic examinations for the early detection of disease: applications to breast cancer. J Am Stat Assoc. 1998;93:1271–1281.
-
- Lee SJ, Zelen M. A stochastic model for predicting the moartlity of breast cancer. J Natl Cancer Inst Monogr. 2006;36:79–86. - PubMed
-
- Lee SJ, Zelen M. Mortality modeling of early detection program. Biometrics. 2008;64(2):386–395. - PubMed
-
- van Ravesteyn NT, Miglioretti DL, Stout NK, Lee SJ, Schechter CB, Buist DS, Huang H, Heijnsdijk EA, Trentham-Dietz A, Alagoz O, Near AM, Kerlikowske K, Nelson HD, Mandelblatt JS, de Koning HJ. Tipping the balance of benefits and harms to favor screening mammography starting at age 40 years: a comparative modeling study of risk. Ann Intern Med. 2012 May 1;156(9):609–17. - PMC - PubMed
-
- Stout NK, Lee SJ, Schechter CB, Kerlikowske K, Alagoz O, Berry D, Buist DS, Cevik M, Chisholm G, de Koning HJ, Huang H, Hubbard RA, Miglioretti DL, Munsell MF, Trentham-Dietz A, van Ravesteyn NT, Tosteson AN, Mandelblatt JS. Benefits, harms, and costs for breast cancer screening after US implementation of digital mammography. J Natl Cancer Inst. 2014 May 28;106(6) - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
