

Increased cardio-respiratory coupling evoked by slow deep breathing can persist in normal humans
- PMID: 25266396
- PMCID: PMC4252616
- DOI: 10.1016/j.resp.2014.09.013
Increased cardio-respiratory coupling evoked by slow deep breathing can persist in normal humans
Abstract
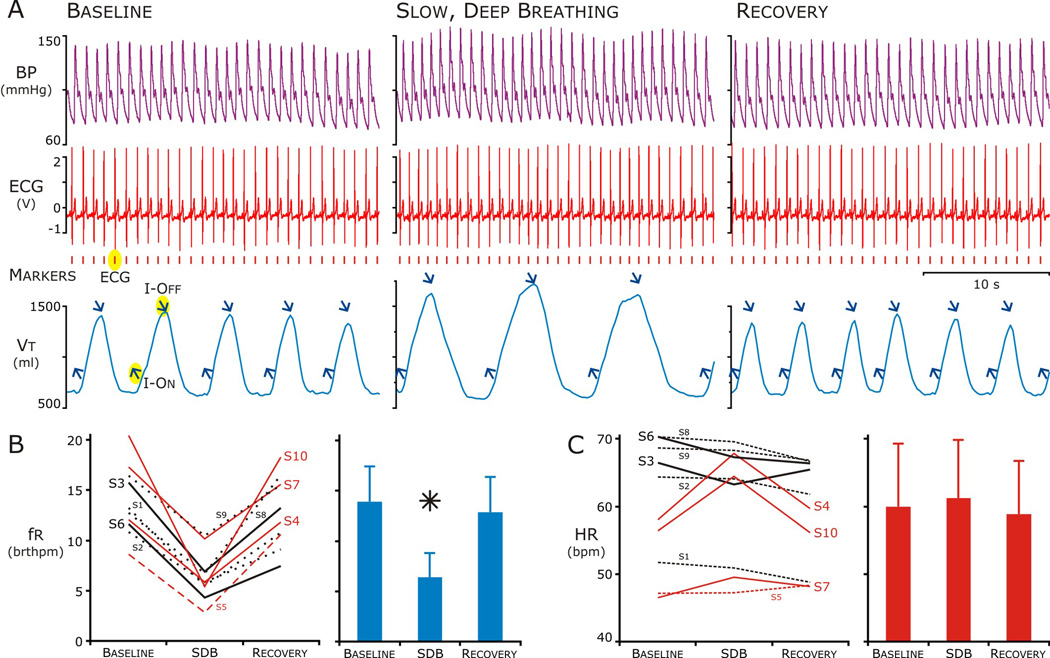
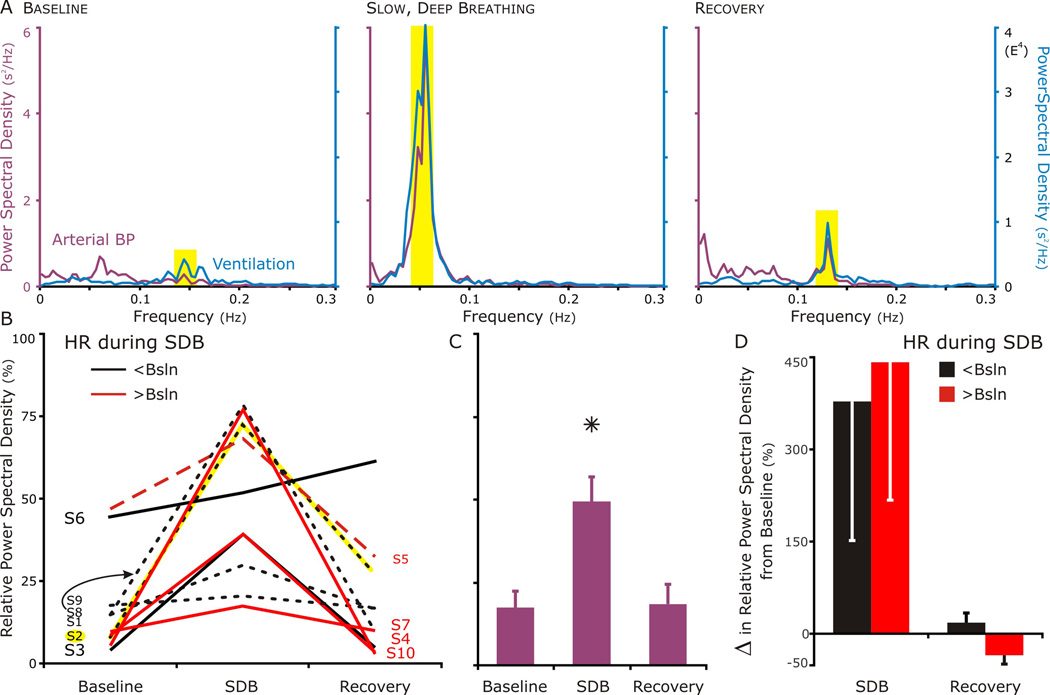
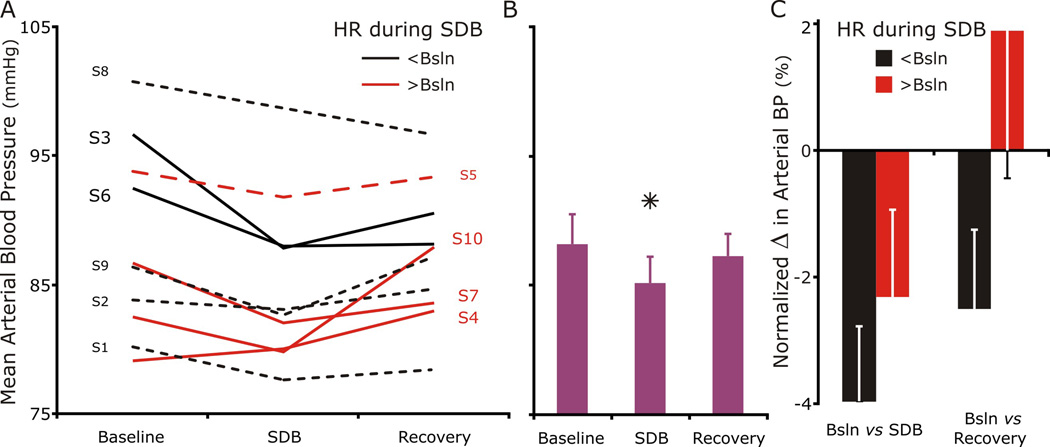
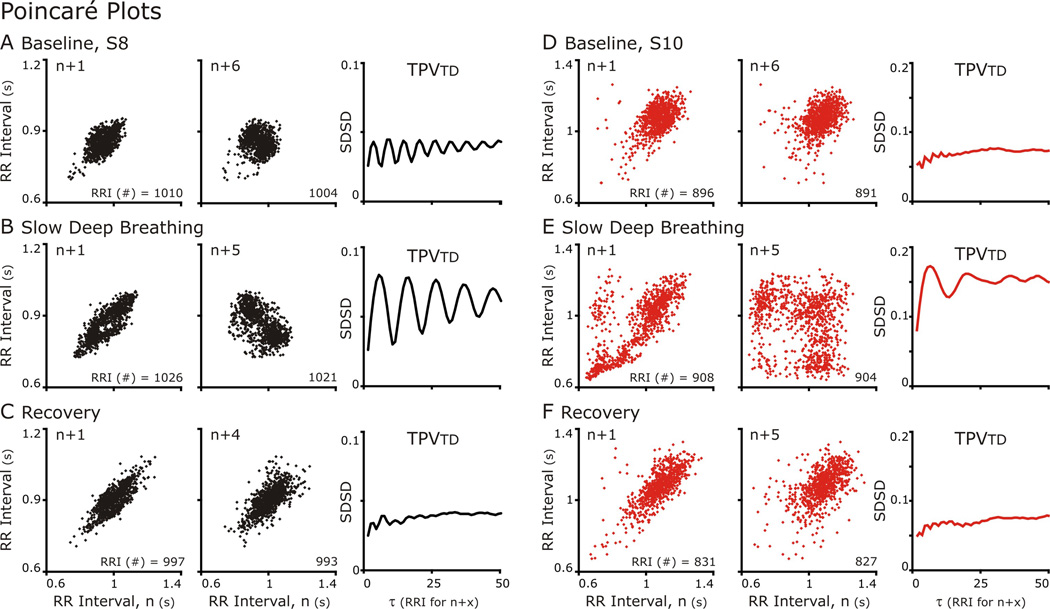
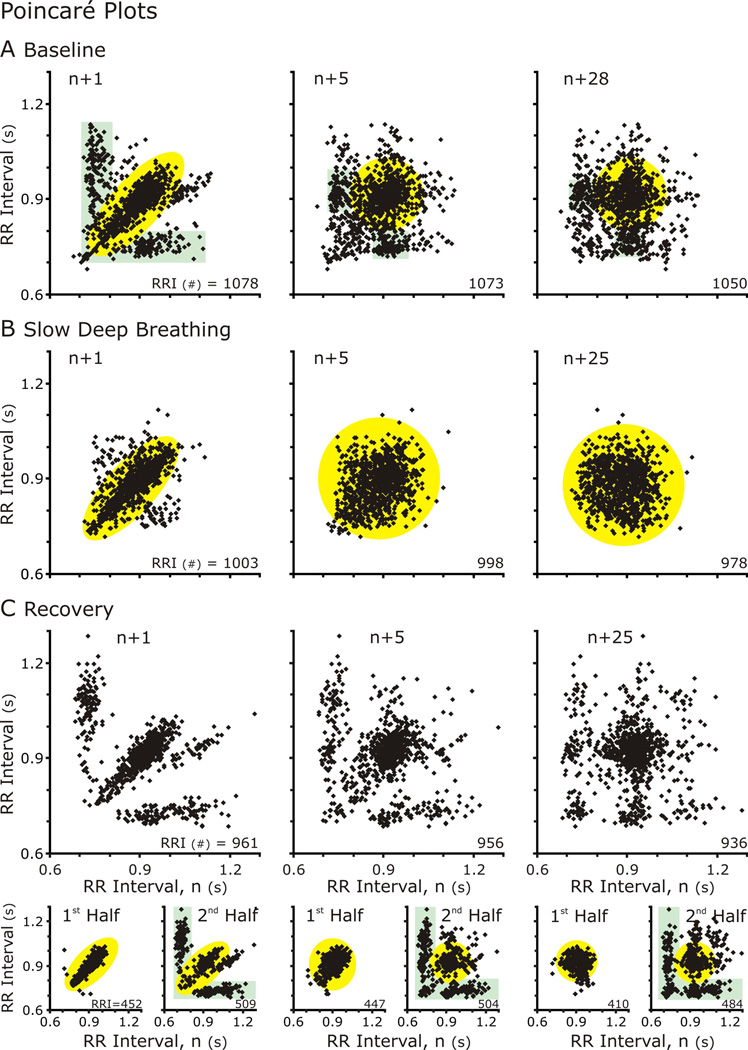
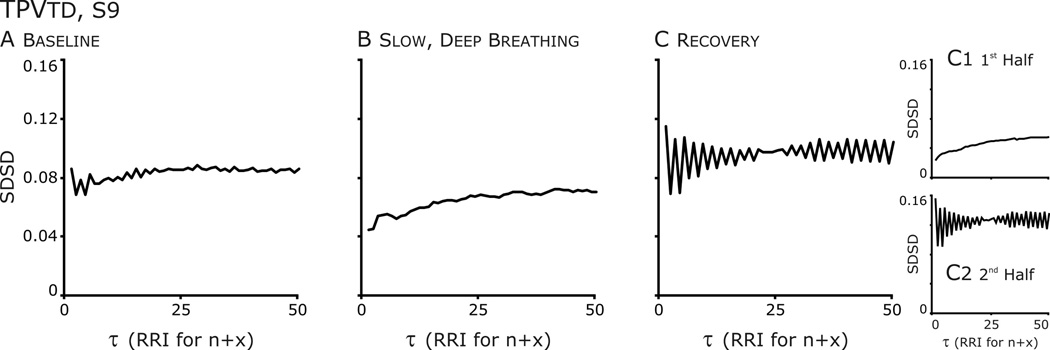
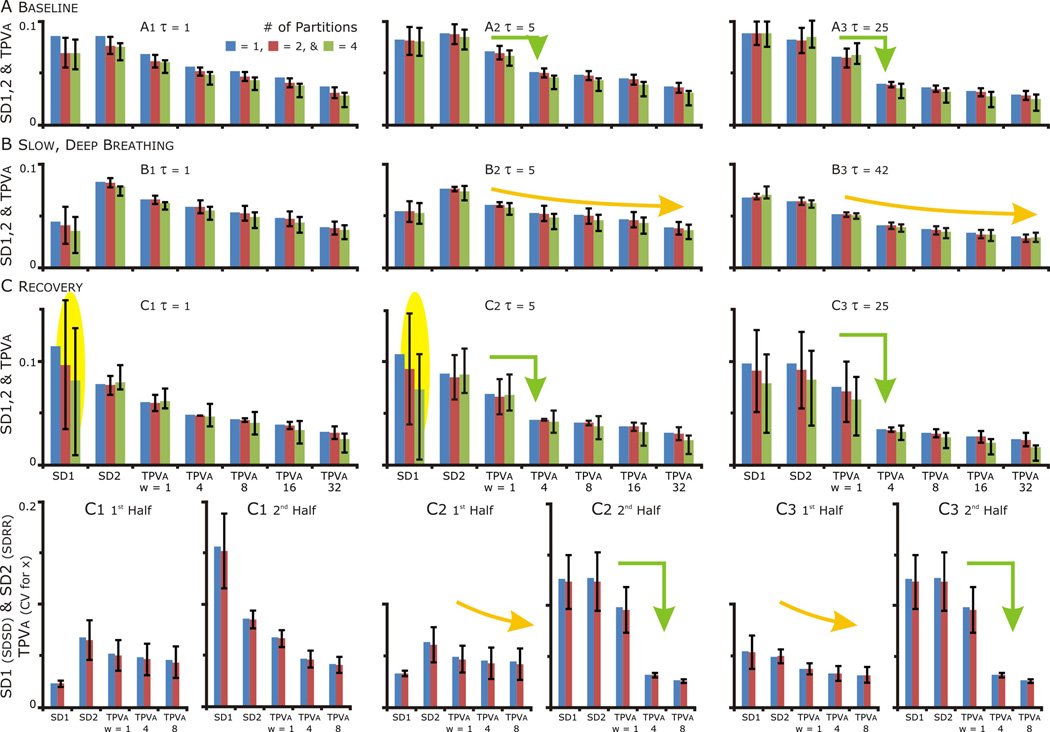
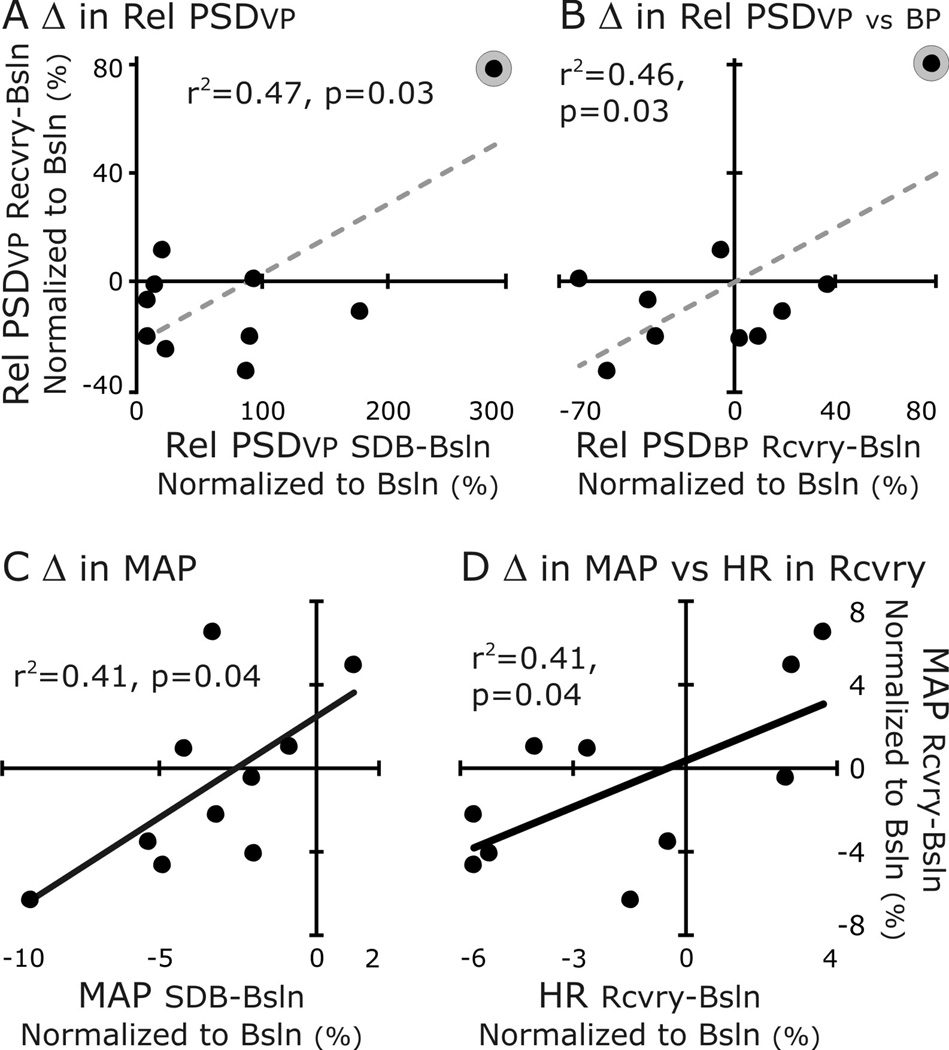
Slow deep breathing (SDB) has a therapeutic effect on autonomic tone. Our previous studies suggested that coupling of the cardiovascular to the respiratory system mediates plasticity expressed in sympathetic nerve activity. We hypothesized that SDB evokes short-term plasticity of cardiorespiratory coupling (CRC). We analyzed respiratory frequency (fR), heart rate and its variability (HR&HRV), the power spectral density (PSD) of blood pressure (BP) and the ventilatory pattern before, during, and after a 20-min epoch of SDB. During SDB, CRC and the relative PSD of BP at fR increased; mean arterial pressure decreased; but HR varied; increasing (n = 3), or decreasing (n = 2) or remaining the same (n = 5). After SDB, short-term plasticity was not apparent for the group but for individuals differences existed between baseline and recovery periods. We conclude that a repeated practice, like pranayama, may strengthen CRC and evoke short-term plasticity effectively in a subset of individuals.
Keywords: Neural control of heart rate; Neural control of respiration; Neural control of sympathetic nerve activity; Poincaré plots; Pranayama.
Copyright © 2014 Elsevier B.V. All rights reserved.
Figures
References
-
- Baekey DM, Dick TE, Paton JF. Pontomedullary transection attenuates central respiratory modulation of sympathetic discharge, heart rate and the baroreceptor reflex in the in situ rat preparation. Exp Physiol. 2008;93:803–816. - PubMed
-
- Bar KJ, Boettger MK, Schulz S, Neubauer R, Jochum T, Voss A, Yeragani VK. Reduced cardio-respiratory coupling in acute alcohol withdrawal. Drug Alcohol Depend. 2008;98:210–217. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
