

Cost effectiveness of the NHS breast screening programme: life table model
- PMID: 23661112
- PMCID: PMC3649817
- DOI: 10.1136/bmj.f2618
Cost effectiveness of the NHS breast screening programme: life table model
Erratum in
- BMJ. 2013;346:f3822
Abstract
Objective: To assess the overall cost effectiveness of the NHS breast screening programme, based on findings of the Independent UK Panel on Breast Cancer Screening and taking into account the uncertainty of associated estimates of benefits, harms, and costs.
Design: A life table model comparing data from two cohorts.
Setting: United Kingdom's health service.
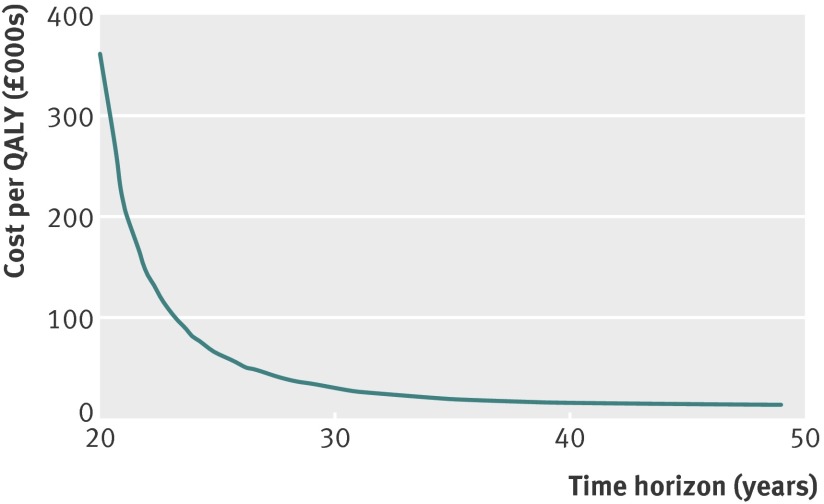
Participants and interventions: 364,500 women aged 50 years-the population of 50 year old women in England and Wales who would be eligible for screening-were followed up for 35 years without screening, compared with a similar cohort who had regular mammographic screening between ages 50 and 70 years and were then followed for another 15 years.
Main outcome measures: Between the cohorts, we compared the number of breast cancer diagnoses, number of deaths from breast cancer, number of deaths from other causes, person years of survival adjusted for health quality, and person years of survival with breast cancer. We also calculated the costs of treating primary and end stage breast cancer, and the costs of screening. Probabilistic sensitivity analysis explored the effect of uncertainty in key input parameters on the model outputs.
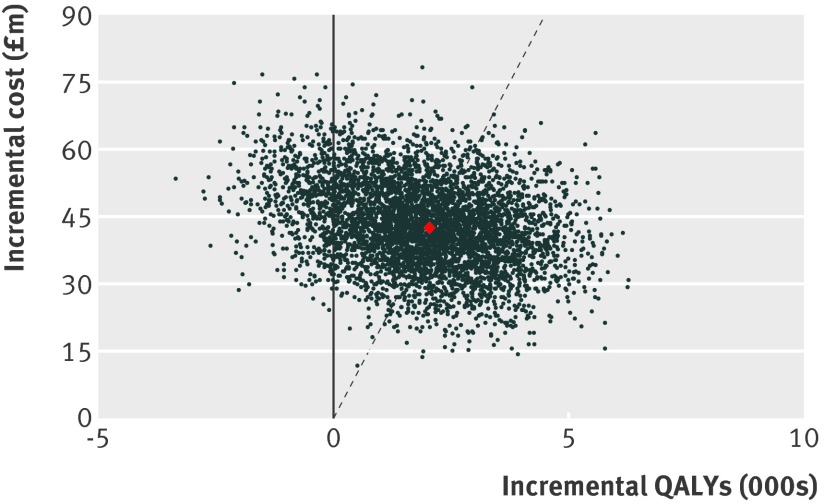
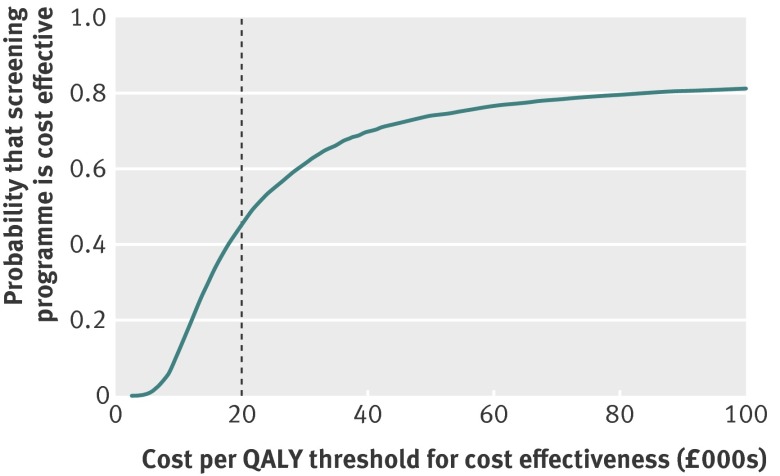
Results: Under the base case scenario (using input parameters derived from the Independent Panel Review), there were 1521 fewer deaths from breast cancer and 2722 overdiagnosed breast cancers. Discounting future costs and benefits at a rate of 3.5% resulted in an additional 6907 person years of survival in the screened cohort, at a cost of 40,946 additional years of survival after a diagnosis of breast cancer. Screening was associated with 2040 additional quality adjusted life years (QALYs) at an additional cost of £42.5m (€49.8m; $64.7m) in total or £20,800 per QALY gained. The gain in person time survival over 35 years was 9.2 days per person and 2.7 quality adjusted days per person screened. Probabilistic sensitivity analysis showed that this incremental cost effectiveness ratio varied widely across a range of plausible scenarios. Screening was cost effective at a threshold of £20,000 per QALY gained in 2260 (45%) scenarios, but in 588 (12%) scenarios, screening was associated with a reduction in QALYs.
Conclusion: The NHS breast screening programme is only moderately likely to be cost effective at a standard threshold. However, there is substantial uncertainty in the model parameter estimates, and further primary research will be needed for cost effectiveness studies to provide definitive data to inform policy.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Estimating the cost-effectiveness of modern screening mammography programmes.Evid Based Med. 2014 Apr;19(2):80. doi: 10.1136/eb-2013-101433. Epub 2013 Sep 24. Evid Based Med. 2014. PMID: 24065863 No abstract available.
References
-
- Forrest APM. Breast cancer screening: report to the health ministers of England, Wales, Scotland, and Northern Ireland by a working group. Department of Health and Social Security, 1987.
-
- International Agency for Research on Cancer. Handbook of cancer prevention: breast cancer screening, volume 7. IARC, 2002.
-
- Woolf SH. The 2009 breast cancer screening recommendations of the US Preventive Services Task Force. JAMA 2010;303:162-3. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical