

Diaphragm postural function analysis using magnetic resonance imaging
- PMID: 23516397
- PMCID: PMC3597716
- DOI: 10.1371/journal.pone.0056724
Diaphragm postural function analysis using magnetic resonance imaging
Abstract
We present a postural analysis of diaphragm function using magnetic resonance imaging (MRI). The main aim of the study was to identify changes in diaphragm motion and shape when postural demands on the body were increased (loading applied to a distal part of the extended lower extremities against the flexion of the hips was used). Sixteen healthy subjects were compared with 17 subjects suffering from chronic low back pain and in whom structural spine disorders had been identified. Two sets of features were calculated from MRI recordings: dynamic parameters reflecting diaphragm action, and static parameters reflecting diaphragm anatomic characteristics. A statistical analysis showed that the diaphragm respiratory and postural changes were significantly slower, bigger in size and better balanced in the control group. When a load was applied to the lower limbs, the pathological subjects were mostly not able to maintain the respiratory diaphragm function, which was lowered significantly. Subjects from the control group showed more stable parameters of both respiratory and postural function. Our findings consistently affirmed worse muscle cooperation in the low back pain population subgroup. A clear relation with spinal findings and with low back pain remains undecided, but various findings in the literature were confirmed. The most important finding is the need to further address various mechanisms used by patients to compensate deep muscle insufficiency.
Conflict of interest statement
Figures
 .
.
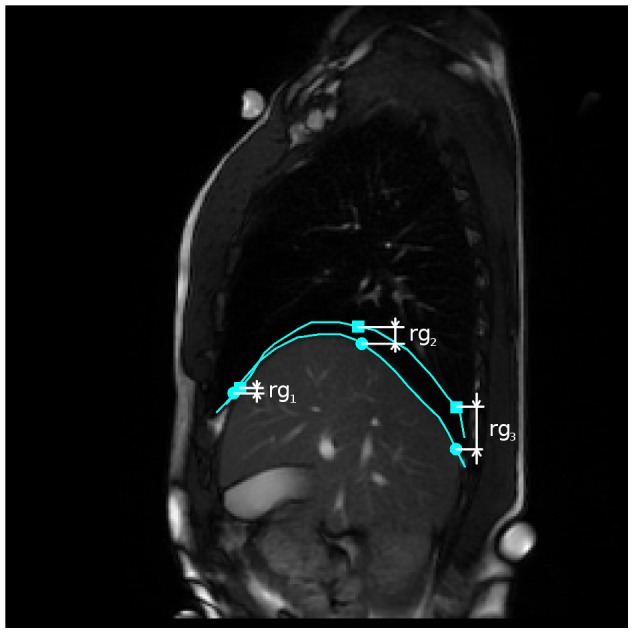
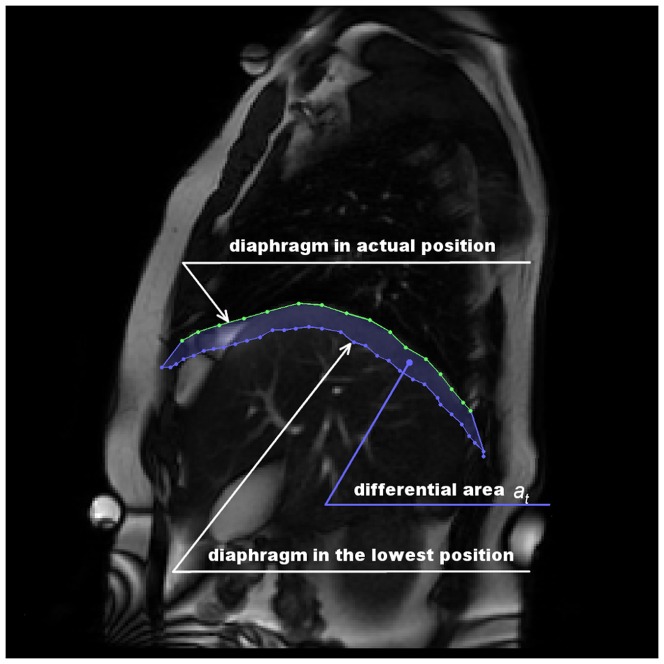
 are computed as vertical subtraction of caudal from cranial diaphragm position. The three parameters correspond to the anterior (
are computed as vertical subtraction of caudal from cranial diaphragm position. The three parameters correspond to the anterior ( ), middle (
), middle ( ) and posterior (
) and posterior ( ) diaphragm part. Points were spread evenly on the diaphragm contour with small constant drift of
) diaphragm part. Points were spread evenly on the diaphragm contour with small constant drift of  and
and  from the contour margins.
from the contour margins.
References
-
- Lewit K (1980) Relation of faulty respiration to posture and with clinical implications. The Journal of the American Osteopathic Association 525–529. - PubMed
-
- Barr KP, Griggs M, Cadby T (2005) Lumbar stabilization: Core concepts and current literature, part 1. American journal of physical medicine and rehabilitation 473–480. - PubMed
-
- Hodges PW, Richardson CA (1999) Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Archives of physical medicine and rehabilitation 1005–1012. - PubMed
-
- Cholewicki J, Ivancic PC, Radebold A (2002) Can increased intra-abdominal pressure in humans be decoupled from trunk muscle co-contraction during steady state isometric exertions? European journal of applied physiology 127–133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
