

Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: Preventing breast cancer
- PMID: 20404000
- PMCID: PMC2935331
- DOI: 10.1158/1940-6207.CAPR-10-0076
Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: Preventing breast cancer
Abstract
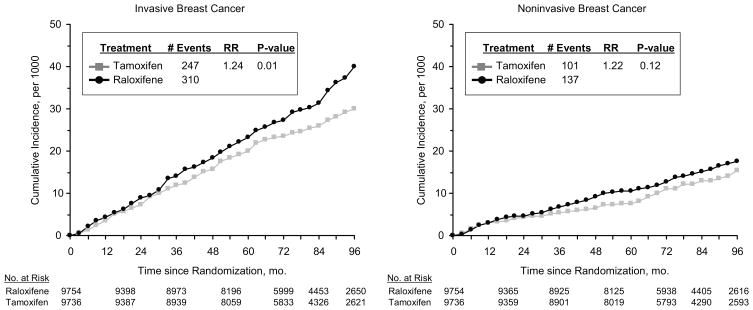
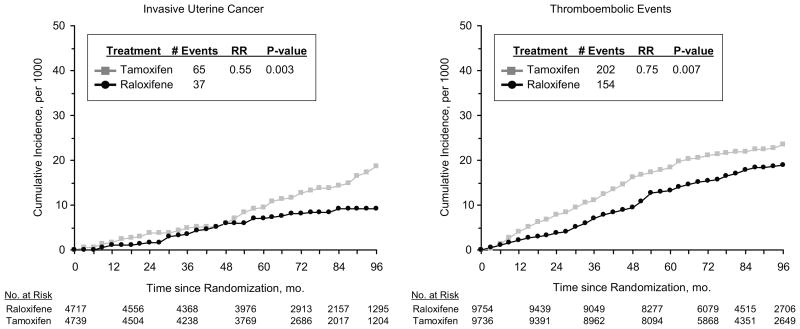
The selective estrogen-receptor modulator (SERM) tamoxifen became the first U.S. Food and Drug Administration (FDA)-approved agent for reducing breast cancer risk but did not gain wide acceptance for prevention, largely because it increased endometrial cancer and thromboembolic events. The FDA approved the SERM raloxifene for breast cancer risk reduction following its demonstrated effectiveness in preventing invasive breast cancer in the Study of Tamoxifen and Raloxifene (STAR). Raloxifene caused less toxicity (versus tamoxifen), including reduced thromboembolic events and endometrial cancer. In this report, we present an updated analysis with an 81-month median follow-up. STAR women were randomly assigned to receive either tamoxifen (20 mg/d) or raloxifene (60 mg/d) for 5 years. The risk ratio (RR; raloxifene:tamoxifen) for invasive breast cancer was 1.24 (95% confidence interval [CI], 1.05-1.47) and for noninvasive disease, 1.22 (95% CI, 0.95-1.59). Compared with initial results, the RRs widened for invasive and narrowed for noninvasive breast cancer. Toxicity RRs (raloxifene:tamoxifen) were 0.55 (95% CI, 0.36-0.83; P = 0.003) for endometrial cancer (this difference was not significant in the initial results), 0.19 (95% CI, 0.12-0.29) for uterine hyperplasia, and 0.75 (95% CI, 0.60-0.93) for thromboembolic events. There were no significant mortality differences. Long-term raloxifene retained 76% of the effectiveness of tamoxifen in preventing invasive disease and grew closer over time to tamoxifen in preventing noninvasive disease, with far less toxicity (e.g., highly significantly less endometrial cancer). These results have important public health implications and clarify that both raloxifene and tamoxifen are good preventive choices for postmenopausal women with elevated risk for breast cancer.
Trial registration: ClinicalTrials.gov NCT00003906.
2010 AACR.
Figures
Comment in
-
Two good choices to prevent breast cancer: great taste, less filling.Cancer Prev Res (Phila). 2010 Jun;3(6):681-5. doi: 10.1158/1940-6207.CAPR-10-0101. Cancer Prev Res (Phila). 2010. PMID: 20522797
-
The lack, need, and opportunities for decision-making and informational tools to educate primary-care physicians and women about breast cancer chemoprevention.Cancer Prev Res (Phila). 2010 Jun;3(6):686-8. doi: 10.1158/1940-6207.CAPR-10-0100. Cancer Prev Res (Phila). 2010. PMID: 20522798
-
Long-term follow-up in cancer prevention trials (It ain't over 'til it's over).Cancer Prev Res (Phila). 2010 Jun;3(6):689-91. doi: 10.1158/1940-6207.CAPR-10-0096. Cancer Prev Res (Phila). 2010. PMID: 20522799 Free PMC article.
-
Breast cancer prevention: an update of the STAR trial.Curr Treat Options Oncol. 2010 Dec;11(3-4):66-9. doi: 10.1007/s11864-010-0124-2. Curr Treat Options Oncol. 2010. PMID: 21061192 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–717. - PubMed
-
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371–88. - PubMed
-
- Cuzick J, Forbes J, Edwards R, et al. First results from the International Breast Cancer Intervention Study (IBIS-1): a randomised prevention trial. Lancet. 2002;360:817–24. - PubMed
-
- Cuzick J, Powles T, Veronesi U, et al. Overview of the main outcomes in breast cancer prevention trials. Lancet. 2003;361:296–300. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
