

Overdiagnosis and overtreatment of breast cancer: microsimulation modelling estimates based on observed screen and clinical data
- PMID: 16524452
- PMCID: PMC1413979
- DOI: 10.1186/bcr1369
Overdiagnosis and overtreatment of breast cancer: microsimulation modelling estimates based on observed screen and clinical data
Abstract
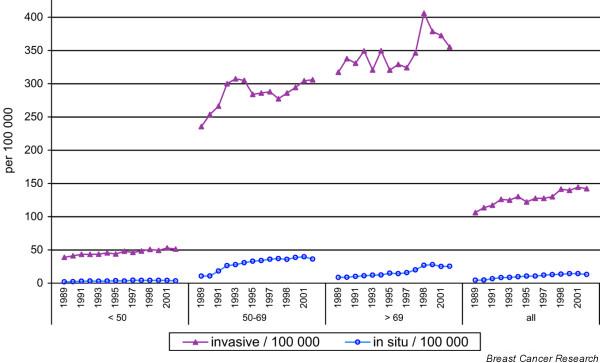
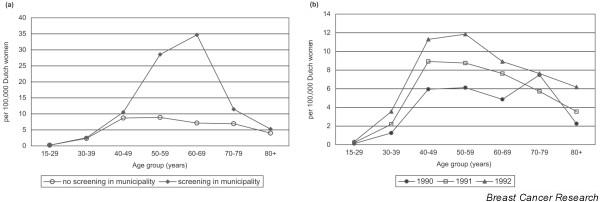
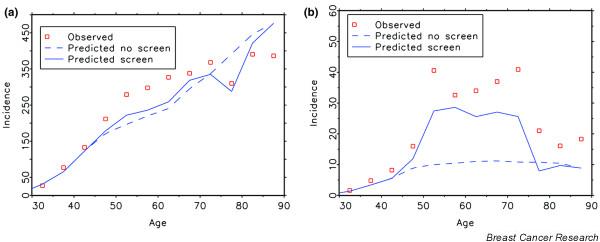
There is a delicate balance between the favourable and unfavourable side-effects of screening in general. Overdiagnosis, the detection of breast cancers by screening that would otherwise never have been clinically diagnosed but are now consequently treated, is such an unfavourable side effect. To correctly model the natural history of breast cancer, one has to estimate mean durations of the different pre-clinical phases, transition probabilities to clinical cancer stages, and sensitivity of the applied test based on observed screen and clinical data. The Dutch data clearly show an increase in screen-detected cases in the 50 to 74 year old age group since the introduction of screening, and a decline in incidence around age 80 years. We had estimated that 3% of total incidence would otherwise not have been diagnosed clinically. This magnitude is no reason not to offer screening for women aged 50 to 74 years. The increases in ductal carcinoma in situ (DCIS) are primarily due to mammography screening, but DCIS still remains a relatively small proportion of the total breast cancer problem.
Figures
References
-
- Otto SJ, Fracheboud J, Looman CWN, Broeders MJM, Boer R, Hendriks JHCL, Verbeek ALM, de Koning HJ, the National Evaluation Team for Breast Cancer Screening Initiation of population-based mammography screening in Dutch municipalities and effect on breast-cancer mortality: a systematic review. Lancet. 2003;361:1411–1417. doi: 10.1016/S0140-6736(03)13132-7. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
